A 36 yr old male with pain abdomen
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.A 36 year old male , cement factory worker residing in nalgonda has come on 18/6/22 with
CHIEF COMPLAINTS:
Pain abdomen since 5 days
HISTORY OF PRESENT ILLNESS :
Patient was apparently asymptomatic 1 yr back and then he developed pain abdomen for which he consulted local practitioner and was diagnosed to have Renal calculi and was given treatment and got relieved.
He now complains of pain abdomen in right loin radiating to right groin since 5 days and for which he consulted local practitioner and took medication .
But the pain is not relieved
And pain is also associated with decreased urine output and abdominal distention.
He then came to KIMS.
No History of fever ,vomiting, loosestools.
CHIEF COMPLAINTS:
Pain abdomen since 5 days
HISTORY OF PRESENT ILLNESS :
Patient was apparently asymptomatic 1 yr back and then he developed pain abdomen for which he consulted local practitioner and was diagnosed to have Renal calculi and was given treatment and got relieved.
He now complains of pain abdomen in right loin radiating to right groin since 5 days and for which he consulted local practitioner and took medication .
But the pain is not relieved
And pain is also associated with decreased urine output and abdominal distention.
He then came to KIMS.
No History of fever ,vomiting, loosestools.
PAST HISTORY :
Patient is not a known case of Diabetes, Hypertension, Epilepsy, Asthma, Tuberculosis .
PERSONAL HISTORY:
Daily routine
Wakes up at 5:30 AM
Breakfast by 7: 30AM
Goes to work
Lunch at 1 PM
Comes home at 5:30 PM
Dinner by 8:30PM
And sleeps at 9 PM
Patient went to the work for first 2 days because the pain was mild
Since it was severe in the next few days he stopped working .
Addictions : Alcohol since 15 years
Twice a week ,180ml
Diet : mixed
Appetite: normal
Bowel and bladder movements: regular
Sleep: adequate
FAMILY HISTORY:
not significant
GENERAL EXAMINATION:
Patient is conscious ,coherent and cooperative
Moderately built and moderately nourished
Well oriented to time place and person
No pallor , cyanosis, clubbing, lymphadenopathy, edema
Icterus present
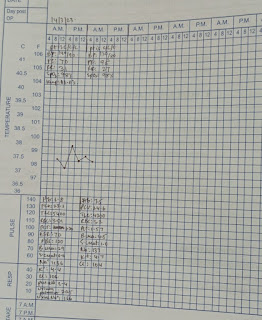
VITALS:
TEMP- Afebrile
BP- 120/90mm hg
PR- 76bpm
RR- 28cpm
SYSTEMIC EXAMINATION:
CVS - S1 S2 heard ,no murmurs
RS- BAE+, NVBS
CNS- NAD
PA-
Inspection:
Abdomen is distended
Umbilicus - normal
Movements - moves with respiration
Skin smooth and shiny
No scars, sinuses, striae, distended veins
Palpation
No local rise of temp
No tenderness
Guarding present
Rigidity absent
Fluid thrill absent
Spleen, liver ,kidneys not palpable
Lymph nodes not palpable












PROVISIONAL DIAGNOSIS
TREATMENT
Inj Piptaz 2.25gm IV BD
IVF NS @50ml/hr
Inj Lasix 40mg IV BD
Inj Pan 40mg IV BD
Inj Zofer 4mg IV TID
Inj Buscopan 1amp IV
Syp Lactulose
Tab rantac
Tab udiliv 300mg BD

Comments
Post a Comment